.svg)

.jpg)
When we think of malaria, familiar images come to mind: feverish patients in clinics, billowing mosquito nets, and rural communities waging a silent battle against a deadly and ancient disease. But one image rarely takes center stage - that of a pregnant woman.
For too long, malaria in pregnancy (MiP) has been an invisible burden in the Asia Pacific region. However each year, millions of women in Asia Pacific are exposed to the dual risks of pregnancy and malaria, a combination that poses significant health threats to both the mother and her unborn child. Particularly in Papua New Guinea and the Solomon Islands where malaria is widespread, pregnant women are among the hardest hit.
MiP has been silently unfolding in clinics and at home for far too long, often lacking the urgency it deserves. MiP is associated with adverse pregnancy outcomes including severe anaemia, miscarriage, stillbirth, preterm delivery, as well as low birth weight which increases the risk of infant death. Yet, national malaria programmes often place more emphases on the visible faces of malaria — children, men in high-risk occupations, or even other communicable diseases. Consequently, women, especially those in their most vulnerable stage of life and carrying the promise of tomorrow, are left behind.
Why has MiP been overlooked?
Historically, pregnant women were excluded from clinical trials for ethical reasons. While well-intentioned, this safeguard inadvertently led to a critical gap in evidence on the safety and efficacy of malaria treatments for pregnant women. Over time, pregnant women were left in a blind spot where delays, uncertainties, and missed opportunities in accessing malaria treatments became the norm. While the world moved forward with effective treatments and renewed hope, expectant mothers remained on the sidelines, despite needing them the most.
Apart from the weight of unchangeable history, another force is at play: how priorities are set in malaria programmes. In Asia Pacific, malaria programmes often centre around the most visible drivers of malaria transmission – mostly men in high-risk occupations, such as forest workers or migrant and mobile populations. Meanwhile, pregnant women whose infections are frequently asymptomatic and whose diagnoses are commonly missed during routine antenatal care, remain unseen in the shadows, further compounding their vulnerability in the very systems meant to protect them.
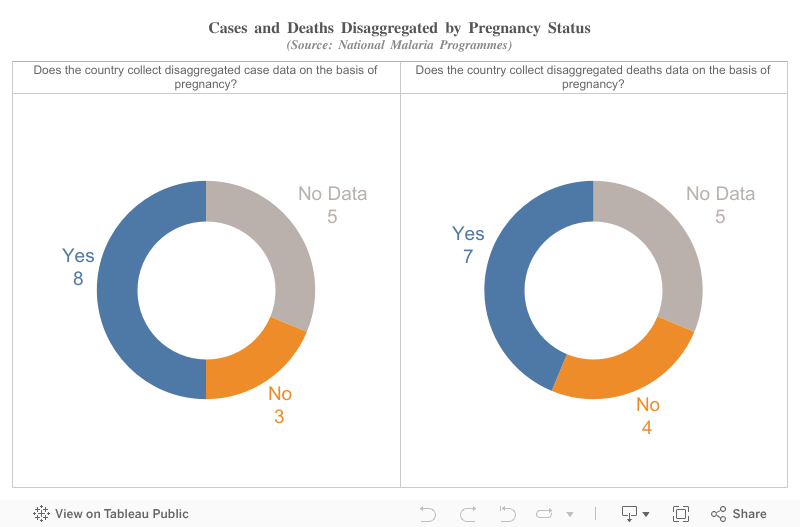
The chart below presents an overview of the availability of pregnancy-related disaggregated case and death data for malaria in the region.
Signs of change
However, some countries in Asia Pacific have taken decisive actions throughout the years to close the intervention gap in MiP.
Papua New Guinea took a bold step of introducing intermittent preventive treatment in pregnancy (IPTp) using sulfadoxine-pyrimethamine (SP) to tackle MiP, a treatment regimen which the World Health Organization currently recommends for use in Africa only. Despite the unconventional approach, results from domestic clinical trials in recent years have supported the potential benefits of IPTp-SP in Papua New Guinea, where it has been shown to reduce adverse pregnancy outcomes in low transmission areas like Port Moresby, as well as conferring protection to other communicable diseases, especially sexually transmitted infections.
Across the ocean, Indonesia has similarly implemented pregnancy-specific malaria strategies, among which includes one-time malaria screening during antenatal care visits and preventive treatment with new drug combinations. In Thailand, proactive weekly screening of pregnant women in temporary shelters along the Thai-Myanmar border has led to a significant reduction in malaria-related maternal deaths. These interventions set the tone for a shift in malaria strategies in the region, advancing towards a future where no pregnant woman is left unprotected against malaria.
Elsewhere across Asia Pacific, countries like Bangladesh, India, Nepal, Pakistan, and Vanuatu have adapted their vector control strategies to include universal or risk-based provisions of insecticide-treated nets (ITNs) to expectant mothers during antenatal care visits. New technological approaches, like the delivery of medical supplies by drone to remote communities, and the use of SMS reminders to help pregnant women keep up with preventive treatments, are catalysing the fight against malaria in the region.
Challenges we cannot ignore
Still, progress remains uneven. Access to ITNs continues to be inadequate for many women in the region, even in countries where widespread ITNs distributions are in place. The uptake of preventive treatments remains low, particularly among remote communities. Health workers lack consistent, clear guidelines on what is safe and effective to prescribe during pregnancy. Furthermore, the diagnostic tools in use today lack the sensitivity to detect infections in asymptomatic women.
Beyond these technical gaps lies deeper, socially entrenched barriers. Poverty, physical distance from health facilities, cultural norms, and lack of decision-making power continue to keep pregnant women away from receiving the malaria prevention and treatment they need. Unless women’s voices are heard, and solutions rooted in their realities, true progress in eliminating malaria will remain uneven and those most at risk will continue to be left behind.
Why inclusion matters
Malaria elimination is not just about bringing the numbers down or shrinking the malaria map, it is a commitment to creating a healthier, more equitable malaria-free future for people in Asia Pacific. Addressing MiP is thus not only a public health imperative, but also a crucial and indispensable step towards advancing health equity and social justice.
Addressing MiP generates far-reaching and long-lasting returns. It leads to improved maternal and neonatal health outcomes, reduces the financial burden and disruptions to livelihoods on families, and contributes to the development of more resilient communities.
The way forward
The Asia Pacific region stands at a defining moment. By strategically investing in research, cross-border collaboration, and malaria strategies that reflect women’s needs, we have a real opportunity to turn the tide on MiP. To move towards this goal, the region must invest their efforts in:
- Expanding surveillance to better understand the true burden of MiP;
- Supporting community-based delivery of preventive treatments that reaches women and expectant mothers effectively;
- Testing and adopting new diagnostic tools that can detect malaria infections earlier;
- Ensuring that women’s voices shape the design of services and communication campaigns.
Above all, it means recognising that pregnant women are not just another “at-risk group". They are central to our vision of a malaria-free future, and their inclusion is indispensable to turning that vision into reality.
A call to action
MiP should not be an inevitable fate for women in the region. Tangible progress in addressing MiP will require strong political will, sustained investment, coordinated efforts across sectors, and a region-wide commitment to ensuring women’s inclusion at the core of malaria elimination strategies. By prioritizing MiP, we can safeguard the health of women and the promises of tomorrow, strengthen communities, and advance decisively towards a malaria-free Asia Pacific for all.
Every mother and child deserves protection, regardless of where they live or what barriers they face.







